Artificial Intelligence is not the end of the doctor. It is the end of a certain way of being a doctor.
4 May , 2026
For months, the most powerful voices in Silicon Valley have been repeating the same prediction: doctors are on their way out, medical schools will become “useless,” and artificial intelligence will make clinicians superfluous.
These claims come from entrepreneurs who have never examined a patient. They are echoed by those who see the healthcare industry—one of the world’s richest markets—as the next great frontier to conquer.
But their message lands loud and clear with a generation that is right now deciding whether to enter medicine.
At the same time, a significant part of real medicine—the kind practiced for decades by those who have seen every new technology of the last forty years enter the wards—is skeptical. And it has serious reasons. Every recent technological innovation has been captured by the logic of volume and productivity, reducing, not increasing, time for patient care. There is no automatic reason to believe artificial intelligence will be different.
The article we just published in JAMA, the Journal of the American Medical Association—one of the world’s most authoritative medical journals (doi:10.1001/jama.2026.4356)—starts precisely from this paradox. It offers a different reading from both Silicon Valley’s triumphant narrative and the understandable pessimism of those who see yet another missed opportunity.
The finding that made the most noise is about empathy.
In blinded studies, written responses from chatbots—programs you can dialogue with in writing—were judged more empathetic than those from doctors in oncology, neurology, mental health, and general medicine. The difference is large, replicated, and shocking to many. But it doesn’t mean what Silicon Valley tycoons want us to believe. A chatbot doesn’t examine a patient, doesn’t read a facial expression, doesn’t carry out a care plan amid uncertainty. The data says something else, and far more serious: medicine has drifted so far from the patient that a system trained on text, facing a screen, can now seem more present than someone who studied ten years to be that.
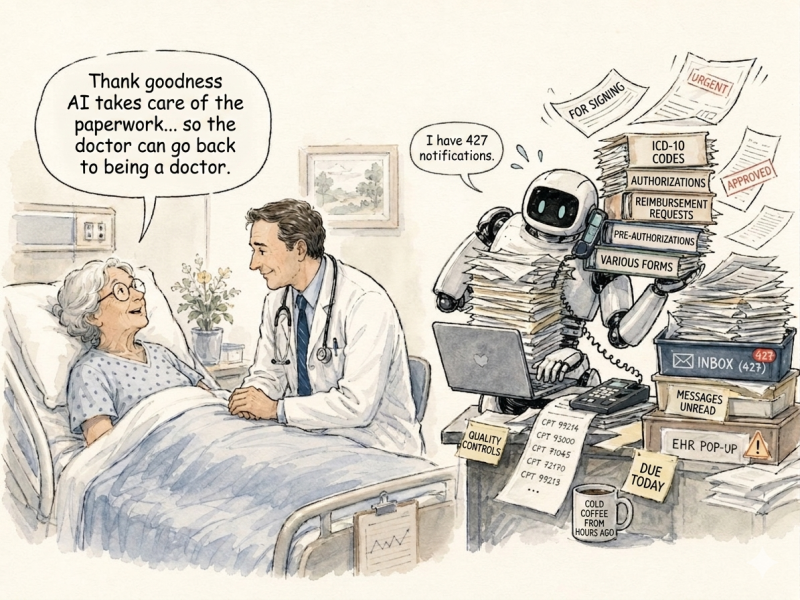
The numbers confirm it. In the United States, physician burnout stands at 45.2%, after peaking at 62.8% during the pandemic: returning to pre-pandemic levels isn’t a solution—it’s proof the crisis is structural. Doctors spend 49% of their outpatient day on electronic health records and desk work, versus 27% in direct patient contact. It’s not just an American problem: the World Health Organization and the OECD report similar issues across Europe.
Let’s say it clearly: the last fifteen years have given patients more than any other period in the history of medicine. Diagnoses once impossible, therapies once unimaginable, survivals no doctor from the previous generation would have believed. The value of being a patient has never been higher. But the job of being a doctor has worsened. Both are true, and our thesis is that we are not forced to keep choosing between them.
At this point, the question becomes: who is really at risk of being replaced by artificial intelligence? Not the doctor themselves. But the doctor reduced to a clerk. The clinician whose day is consumed by documentation, coding, authorizations, and email management is already partially replaceable, because that’s exactly what AI does best. The doctor who no longer looks at the patient, because the system doesn’t allow it, is the most exposed. Not through their own fault, but because a structure has slowly turned them into a data operator.
There’s a second, more urgent front: residents. The PERFORM study, conducted by our group and published last year in Mayo Clinic Proceedings: Digital Health, showed that large language models match or surpass doctors in training in diagnostic accuracy under time pressure—the very condition where human reasoning degrades. If residents are used to fill charts, clear bureaucratic tasks, and oversee billing codes, we are training a generation on activities that AI performs faster than they do. Everything that will make them irreplaceable—clinical reasoning, physical exams, the ability to stay with the patient in uncertainty—is exactly what current training compresses.
The deepest wound isn’t organizational. It’s vocational. Administrative medicine has eroded the doctor’s autonomy, reduced expertise to an exercise in compliance, placed a screen between clinician and patient. The condition that made medicine a vocation has vanished. People still enter this profession for the same reasons as always—to stay beside those who suffer—but they end up doing a different job.
This is the point I want to leave with readers, especially doctors. Artificial intelligence isn’t magic. It’s mathematics. It can be specified, built, and governed by those who know it well enough to reject versions that don’t serve patients. Unlike almost all previous technologies, AI doesn’t have to be simply endured: it can be written.
The real question isn’t what AI will do to doctors, but which doctors are building it. If clinicians aren’t the protagonists, someone else will be—and today’s residents, and tomorrow’s patients, will inherit what those others have built.
It’s not fate. It’s a choice.
This is the direction in which, at the Sbarro Health Research Organization at Temple University in Philadelphia, together with collaborations with the University of Siena and the Scuola Superiore Meridionale of Naples, we are orienting our research.
The idea we propose in the article is one of excavation: artificial intelligence shouldn’t build something new on top of medicine; it should remove what has been built on top of the doctor-patient relationship in the previous forty years. By restoring time, it restores the minimum condition for the profession to become a vocation again.
The crossroads is real. If AI is used to accelerate documentation and multiply visits, it will worsen the situation. If it is used to bring the doctor back to the bedside, it can restore to medicine what it has lost. Technology doesn’t choose on its own: doctors, educators, and health systems do. And too often, they do it in their absence.
Young people choosing medicine today do so despite what Silicon Valley tycoons say about the profession’s future. It falls to my generation, and those before me, to prove they made the right choice. The vocation today doesn’t need defending: it needs strengthening. And that’s done by entering, not exiting, the science that’s changing medicine.
Artificial intelligence is not the end of the doctor. If anything, it’s the opportunity to remind us why we became one.
By Prof. Antonio Giordano